The Adaptive Internship Experience: A Perspective from Sydney W.
Sydney W., former Adaptive intern
During the summer and fall of 2020, I had the great pleasure of working as a digital marketing and communications associate on Adaptive Biotechnologies’ Corporate Marketing and Communications Team. My role consisted of creating content to communicate the science behind the company’s immune medicine platform – using social media to share that information broadly. During my time at Adaptive, I came to learn the inextricable connection between clinical medicine, biotechnological advancement, and the patient story. My advice to all incoming interns is this: be open-minded and eager to learn anything and everything you can from those around you. Whatever your desired career trajectory, the lessons you learn and knowledge you acquire while working at Adaptive will carry forward through anything you do.
As a pre-medical student at Vanderbilt University studying Medicine, Health, and Society, I had originally anticipated spending my summer working in a hospital setting to gain clinical exposure. However, the unforeseen circumstances surrounding the onset of COVID-19 restricted my ability to do so, and I began seeking other ways to make a meaningful impact on patients’ lives. I stepped into my role at Adaptive as it turned its technology toward decoding the immune response to COVID-19 and contributing to vaccine research, watching as the urgent relevance of immune medicine became clear to the world at large. As the pandemic response unfolded, I spent my time writing about Adaptive’s discoveries related to COVID-19. Whether explaining the basic workings of the adaptive immune system or describing the vital role of T cells in conferring long-term immunity to SARS-CoV-2, I was comforted knowing my work was augmenting the general public’s understanding and contributing to the fight against the pandemic.
During my time at Adaptive, I became fascinated by the potential of utilizing the immune system as a natural diagnostic and therapeutic tool in biomedical research. I was inspired to continue exploring the impact of immunological discoveries in a clinical setting. When I returned to Vanderbilt’s campus in the Spring of 2021, I began working as an Undergraduate Research Assistant in the Bohannon Lab at Vanderbilt University Medical Center to investigate immunomodulatory therapies for the prevention of infection and sepsis in patients with burn and other critical injuries. In my gap year following graduation and prior to attending medical school, I plan to work as a Research Fellow in the Marciscano Lab at Weill Cornell Medicine to discover and validate novel, effective, and potentially synergistic combinations of radiotherapy and immunotherapy for treating cancer.
As I venture into medical school and beyond, I will carry forward all I’ve learned from working at Adaptive. Effectively translating scientific concepts into digestible information for various audiences honed my science writing and communication skills. As a prospective physician, it’s imperative for me to adapt medical knowledge to connect with patients, allowing for effective treatment. My time at Adaptive taught me that a unique story is unfolding inside every patient’s body. Great physicians know how to both listen to and tell that story.
One thing that stood out for me during that summer – the people. I cannot speak highly enough of the bright, dynamic, and welcoming individuals with whom I worked. They immediately made me feel comforted and supported, which gave me the confidence to live out my potential on the team and make meaningful contributions that built upon my colleagues’ work. Adaptive is an incredible place to explore the promise of immune medicine, partake in groundbreaking biotechnological pursuits to improve patient outcomes, and witness the workings of the healthcare industry.
March 8, 2022
A Message from Co-Founder and CEO Chad Robins
Chad Robins
Earlier today, Adaptive Co-Founder and CEO Chad Robins sent the following note to Adaptive Biotechnologies employees:
Dear Adapters,
I am writing to you today with hard news to share. As many of you are aware, we recently announced a restructuring to create a more streamlined and focused organization with two business units that will best position us for success: MRD and Immune Medicine. As part of this process, we have made the difficult decision to reduce our workforce. This directly impacts approximately 100 current team members.
Personally, this is one of the hardest decisions I have had to make in my 12 years at Adaptive, especially since I have close, personal relationships with several impacted Adapters. I am also confident that this is the right decision. Our vision and mission have been our north star. We are doing something transformative here. This reorganization and the headcount reduction are necessary for us to enable patients to benefit from our game changing technologies in as short a time as possible.
Ensuring we have the capital and the resources to fuel our growth while navigating turbulent market conditions has resulted in the need to make hard choices. This is a business decision but believe me, I know it affects us all very personally.
Focusing and Prioritizing to Drive Growth
Over the past several weeks, the executive team has made decisions to prioritize key product development efforts that will be most impactful to our goals and objectives for each business area. Given current market conditions affecting Adaptive and the biotech industry more broadly, it is also critical to manage our operating expenses and extend our cash horizon.
We performed a comprehensive review of all departments across the company in conjunction with the ongoing reorganization of the business. It became clear that we had to cut operating expenses, deprioritize certain projects and programs, and make significant adjustments to expenditures on capital projects. This decision was a last resort after considering all these alternatives.
Transition Support
I have always told you that I consider our team to be more than just co-workers, and I truly mean it. Each Adapter has played a crucial role in building the vision that we strive towards every day. You have brought talent, knowledge, dedication, and passion to our organization. We have built Adaptive together and your role in helping to create a new category of medicine will be part of your – and all of our – shared legacy.
There is no easy way to share this news or to say goodbye to our colleagues and friends whom we respect and admire. I want you to know that our team is doing everything we can to support all of you during this transition with the utmost compassion and thoughtfulness. All departing colleagues will be receiving a comprehensive exit package comprised of the following elements:
Separation payment based on tenure
2021 Bonus Payout
Continued benefits coverage support through the end of May for those currently enrolled + their dependents
Extended access to the Employee Assistance Program through end of May
Our internal talent acquisition team will offer resume reviews and interview workshops, create a resume book to share across a broad network of companies, and assist with other outplacement support
Execs will help impacted employees to network with other companies
Next Steps
Those of you leaving Adaptive will receive a calendar invite momentarily to a departure meeting with a senior leader in your department. The final working day for departing employees is today, March 8th.
For those of you remaining with Adaptive, you will be hearing from the executive leader on your team today. Tomorrow, we will be holding an all-company meeting to discuss the future of Adaptive and answer questions.
A Final Note
We are parting ways with many extremely talented and dedicated colleagues. We know this is difficult and, for many, will take a long time to process. We will get through this together, and we will be providing resources to help us all navigate this time.
For those who will be leaving us, I want to thank you again for the time and work you have put into Adaptive; we would not be the organization we are today without your dedication and hard work. The contributions, the relationships, and the lessons we have all learned together will endure, and we sincerely hope you are proud to be part of the Adaptive story.
Please reach out if there is any way we can help you as you continue the next part of your journey.
With gratitude,
Chad
February 28, 2022
Molecular Laboratory Operations: The Heartbeat of Adaptive
Adaptive Corporate Marketing and Communications
In this video Barbara Zehentner (VP, Molecular Lab Operations), Mark Adams (Chief Operating Officer), John Alsobrook (Sr. Clinical Lab Director), and our laboratory staff introduce you to the heartbeat of Adaptive Biotechnologies: our Molecular Laboratory Operations.
Learn more about the journey of samples through Adaptive and Adaptive MLO staff by watching the video below:
February 4, 2022
Whatever Happens, the Patient Has to be at the Center
In honor of World Cancer Day, we sat down with two Adapters to understand how their personal experiences with cancer intersect with their work at Adaptive. Kathy Thompson (Key Account Manager, clonoSEQ sales) is a stage 1 colorectal cancer survivor. Shannon Fatigante (Talent Acquisition Senior Program Manager) has a father currently fighting chronic lymphocytic leukemia (CLL).
Shannon: When my dad called me last summer, he very calmly shared that his recent bloodwork had revealed that he had cancer – specifically CLL.
Shannon Fatigante and her Family
In that moment, my whole world slowed down.
I couldn’t believe what I was hearing. Once I collected myself, my brain caught up with me and it registered that he said CLL. Immediately a few things became clear and put my racing mind at ease: 1) We have a test for measuring cancer burden in CLL. 2) There’s longevity with this type of blood cancer. Treatment advancements are being made at an outstanding pace, which meant this could be a chronic condition. I almost immediately reached out to my colleagues on the diagnostic team to learn more about the disease and received so much helpful information, an example of which can be found here.
Kathy was an incredible resource who offered me comfort and reassurance and has continued to check in on me as my father’s journey continues.
Kathy: I was so happy to help. I’ve worked in oncology for nearly 20 years. But I know from experience, being on the patient’s side of things, it’s different. I didn’t understand how different until it happened to me.
Last February, I was diagnosed with colorectal cancer. After two agonizing weeks waiting for test results, I learned that my cancer was stage 1 and operable. I was operated on robotically but was rushed back to the ER within days after going into septic shock, where I coded for 10 minutes. Against the odds, I survived the ordeal and spent two and a half months rehabilitating at the hospital. With my one-year surgery anniversary around the corner, I recently met with the trauma surgeon who saved my life and shared my gratitude.
Kathy Thompson and her Family
Their empathy for me and willingness to go the extra mile made all the difference in my care. As a patient, you have to advocate for yourself or your loved one. I heard at a conference once that patients only retain one quarter of information received during an appointment. I always tell patients I meet to take a notebook to doctor’s appointments, ask to record conversations so you can refer to them later, and don’t delay your colonoscopy!
Shannon: Absolutely. After talking to Kathy and heeding her advice, I’m so much more prepared to be a resource for my dad and his caregiver, even if it’s just as a shoulder to lean on, or a person to vent to without fear of judgement. Recently, my dad was told he needed treatment and after speaking with his doctor, he was able to get tested for minimal residual disease (MRD) so he could better understand what was happening inside his body. Luckily my dad is feeling well today. Having access to information about his minimal residual disease that can potentially guide important care decisions has been an immense comfort to my dad and me.
We’re not lost here.
Kathy: That reassurance is priceless. For me, I have to get a CT and blood work every three months to catch any sort of recurrence. The weeks leading up to those appointments I’m making myself crazy, looking up symptoms and trying to identify if anything feels off.
As a CLL patient tracking his MRD, Shannon’s dad knows that there is a test that can find his cancer in 1 in a million cells, and that’s a whole different kind of relief. I don’t have that kind of reassurance, but I want that for every blood cancer patient.
Shannon: I know you do! You’ve made me feel so understood and proud to work at Adaptive. I’ve always felt so driven by the patient aspect of our work, but now I’m connected to it in a whole different way. I know what we do is helping my dad and others. I know I am helping to recruit and build teams, so this important work is in the right hands, and ultimately helping patients. I meet with diagnostic sales specialists, share my own story, and I can see how the right people connect with me and meet that level of passion, and that attracts them to Adaptive.
Kathy: You aren’t a good oncology rep unless you really care. A huge part of our job is patient advocacy. Shannon and I both know at the end of the day, whatever happens, the patient has to be at the center.
January 14, 2022
Adaptive Computational Biologist Rachel Gittelman on her 2021 STAT Wunderkind Induction
Rachel Gittelman, Adaptive’s Innovation team
Late last year I was honored to be inducted into the STAT Wunderkinds class of 2021. The award honors early-career scientists across academia and industry that are making important contributions to science and healthcare.
I was grateful to learn that my colleagues at Adaptive had nominated me to join this impressive group. Since joining Adaptive as a computational biologist in 2016, my focus has been on synthesizing complex, multi-dimensional immunomics datasets and correlating these with clinically relevant metadata. I have been combining my knowledge of biology, medicine, and statistics to interpret patterns within our immune system, with the goal of developing better diagnostics for patients based on how our immune systems naturally detect disease and respond to therapy.
My current role on the Innovation team is to lead disease modeling research on the Antigen Map. The Antigen Map was established when Adaptive partnered with Microsoft in 2018 to apply machine learning and cloud computing to Adaptive’s deep sequencing technology to decode and map the human immune response to many different diseases. The nature of my work became even more critical during the pandemic. I helped lead a team of Adaptive and Microsoft employees to analyze data from blood samples of over 6,500 people infected with SARS-CoV-2 from all over the world, identifying SARS-CoV-2 associated T-cell receptor sequences and the viral antigens they map to. These data were made available to the research and scientific community via ImmuneCODE – Adaptive and Microsoft’s open public database. Ultimately, this work led to the launch of Adaptive’s first commercially available T-cell test designed to detect recent of prior SARS-CoV-2 infections.
While I’ve known the importance of my work, I became even more proud of my accomplishments following the Wunderkinds virtual meet and greet, where I met the 26 other members of my class, and realized what truly impressive company I’ve found myself in. This year’s trailblazing cohort included researchers working on a wide variety of topics, from machine learning in single-cell cancer diagnostics, to gene editing techniques in sickle cell disease and beta thalassemia, and investigations into the health disparities in BIPOC communities.
As a member of the Wunderkind class of 2021, I was invited to attend STAT’s annual summit, which was virtual this year. The summit featured an impressive list of speakers – from researchers to activists to politicians – who were interviewed by the reporters at STAT. This format was an interesting departure from the types of conferences I’m used to – without slides or figures, just informal conversations with the speakers. Discussion was, of course, dominated by COVID-19, but there were some other topics as well.
Some of my favorite talks included a conversation with Trevor Bedford, PhD, a scientist at the Fred Hutchinson Cancer Research Center and an expert on viral evolution and epidemiology, about the future of the coronavirus. My scientific background before I started at Adaptive was in population genetics, evolution, and phylogenetics, so I was excited to see Trevor Bedford talk, and have been following him on Twitter throughout the pandemic.
I am so grateful to Adaptive’s leadership team for nominating me for this recognition and gifting me this incredible opportunity. It has been an incredible privilege to join this diverse community of up-and-coming scientists. Since the virtual meetup, STAT has also been keeping us connected on LinkedIn and I was excited to learn a few of us are located in Seattle. I am certain I will continue to benefit from these connections I’ve made in the future.
This designation is a reflection of not just my work but the fantastic people I work with. Everything I do at Adaptive is truly a team effort, and I am continually inspired by my colleagues and what we can accomplish together.
I’ve learned so much from leading the Antigen Map work focused on COVID-19 since the beginning of the pandemic. It was thrilling to analyze massive amounts of data from the adaptive immune system in close to real time, to help our team develop new ways to read and interpret the immune system response. I’m excited to see how we can apply this knowledge to other disease states and conditions, like autoimmune disorders and cancer.
January 4, 2022
MRD in Action: Q&A with Dr. Luciano Costa on the MASTER Trial at ASH 2021
Luciano Costa, MD, PhD, Associate Director for Clinical Research at O’Neal Comprehensive Cancer Center & Susan Bobulsky, SVP, Diagnostics, clonoSEQ
Earlier this month, the blood cancer community came together for the American Society of Hematology 63rd Annual Meeting. Susan Bobulsky, SVP of Diagnostics at Adaptive, sat down with Luciano Costa, MD, PhD, Associate Director for Clinical Research at O’Neal Comprehensive Cancer Center, University of Alabama at Birmingham, to discuss the some of the most compelling multiple myeloma data from this year’s meeting, as well as learn more about results from the MASTER trial, which was published online on December 13, 2021 in the Journal of Clinical Oncology.
Data from the MASTER trial supported the cessation of therapy in newly diagnosed multiple myeloma patients who showed deep MRD-negative responses to treatment. This is a consequential study as we continue to study and understand the role of MRD in guiding therapy choices for blood cancer patients and could have meaningful implications on patients’ quality of life by providing an approach to address the toxicities and financial burden associated with long-term treatment.
What data were you most eager to see presented at ASH around minimal residual disease (MRD)?
The MRD data from the CASSIOPEIA trial.CASSIOPEIA compared bortezomib (Velcade), thalidomide, and dexamethasone [VTd] with daratumumab [Darzalex; DARA]–VTd induction followed by transplant followed by VTd or DARA-VTd consolidation, and we learned that patients who received DARA-VTd did very well, although they didn’t benefit from maintenance. Now, we’re looking at MRD data. It was fascinating to see the outcome of DARA-VTd treated patients who achieved MRD negativity and have not received any additional treatment.Those patients are doing incredibly well with a progression-free survival [PFS] rate over 95% with 4 years of follow-up.
What are some of the most promising treatment advances for multiple myeloma (MM) that were discussed at the meeting?
In multiple myeloma, this was an evolutionary rather than a revolutionary meeting. We saw advances in quadruplet therapy in newly diagnosed multiple myeloma (NDMM), more mature data on T-cell engagers and CAR-T cell therapy in the relapsed and refractory setting.
Can you share how MRD is being used as an endpoint in clinical trials for new therapeutic advances, specifically in MM?
In multiple myeloma, MRD is being used mostly as a correlative biomarker. That being said, we are starting to see MRD utility studied in a variety of ways. First, as a primary endpoint (as in the German isatuximab-VRd trial presented at ASH), or to define eligibility (as in the AURIGA trial), or as modifier of therapy (SWOG 1803, MASTER).
Can you discuss the MASTER study and how MRD played a role? What does this data mean for patients?
In the MASTER trial, we wanted to experiment with cessation of therapy in newly diagnosed MM patients with sustained deep MRD responses. We enrolled NDMM patients and treated them with 4 cycles of induction therapy with daratumumab, carfilzomib, lenalidomide, and dexamethasone (Dara-KRd) followed by autologous transplant and Dara-KRd. In the study, the duration of therapy was determined by achievement of minimal residual disease (MRD) endpoints. This treatment regimen was innovative – very few trials use Dara-KRd up front. What was perhaps most notable about this study was that it was the first trial in MM where MRD is used not only as a correlative but as an actionable parameter.
The primary endpoint of the study was MRD-negative remission (<10-5) as defined by International Myeloma Working Group (IMWG) criteria, using next-generation sequencing with clonoSEQ.The primary endpoint was achieved in 80% of the patients. The study also reported that 66% of patients achieved MRD at 10-6.
MRD was assessed utilizing clonoSEQ in 118 patients. Of those, 84 patients (71%) achieved two consecutive MRD-negative results <10-5, which enabled subsequent treatment discontinuation.MRD follow-up for these patients occurred at 6 months after treatment cessation and then on an annual basis. At 12 months post treatment cessation, the risk of MRD resurgence was 4% for patients with standard or high-risk cytogenetic abnormalities.
We could see very early on in the trial that there were deep responses with this regimen. Dara-KRd induction, ASCT and Dara-KRd consolidation guided by MRD was shown to be feasible, with an acceptable safety profile and leading to rapid responses with a high proportion of patients achieving CR/sCR. The data generated from our analysis showed that MRD response-adapted therapy in patients with NDMM allowed confident and successful treatment discontinuation.
clonoSEQ® is available as an FDA-cleared in vitro diagnostic (IVD) test service provided by Adaptive Biotechnologies to detect minimal residual disease (MRD) in bone marrow from patients with multiple myeloma or B-cell acute lymphoblastic leukemia (B-ALL) and blood or bone marrow from patients with chronic lymphocytic leukemia (CLL). clonoSEQ is also available for use in other lymphoid cancers and specimen types as a CLIA-validated laboratory developed test (LDT). For important information about the FDA-cleared uses of clonoSEQ including test limitations, please visit clonoSEQ.com/technical-summary.
December 14, 2021
The Other Side of The Story: Vaccines Must Produce Both Antibodies and T cell Immunity
Harlan Robins, PhD, Chief Scientific Officer and Co-founder
It’s time to include T cells in the fight against COVID-19.
The scientific community brought novel vaccines to the world in less than a year. That heroic work saved millions of lives. These vaccines were designed specifically to induce antibodies that target the spike protein and disable the virus, blocking it from entering the ACE2 receptor on cells.
Like other vaccines, efficacy was largely measured by using tried and true technology — cheap, simple assays that almost any lab around the world can run — to count the number of neutralizing antibodies against the spike protein.
We knew the target (we thought). This strategy worked brilliantly with the original strain – even better than we had hoped.
But much to our surprise, the virus started to mutate faster. Like other coronaviruses, SARS-CoV-2 is a long RNA virus with an enzyme that self-corrects errors in its genetic code. Therefore, we expected it to evolve slowly. Shorter RNA viruses such as influenza or HIV don’t have this error correction capability. They mutate regularly, which makes these viruses especially difficult moving targets for vaccine developers.
Now we know SARS-CoV-2 is a tough adversary for vaccine development. As the virus started mutating and moved through the Greek alphabet, it successfully evaded much of the neutralizing antibody response induced by vaccines or previous infection-induced immunity.
The neutralizing antibody response has fallen off dramatically – a 40-fold drop against the Omicron variant, according to an early report out of South Africa. But that worrisome development hasn’t yet translated into a real-world drop in vaccine efficacy. How could that be?
The current hypothesis is because of the T cell response, the other primary mechanism by which the adaptive immune system fights viruses. Antibodies prevent the virus from entering cells. T cells locate and kill cells that have been infected by a recognizable pathogen.
Evidence has been mounting in recent months demonstrating that T cells bind to more parts of the SARS-CoV-2 virus than antibodies, which makes it much more difficult for the virus to escape killer T-cells, also known as CD8+ T-cells. In fact, T-cell levels are correlating directly with real-world vaccine efficacy.
Sure, there were breakthrough infections by the time the Delta variant swept the world, but thanks to T cells, hospitalization and death rates among vaccinated individuals were extremely low.
Historically, antibodies have been used as the main measure of vaccine response because they are well-understood and easy to measure. As opposed to a simple blood-based serology test to measure antibodies, the traditional methods for measuring the T cell response require functional assays that use live cells. Since live cells are finicky, these assays are virtually impossible to standardize and run at scale. Also, functional assays require samples to be viably frozen, which is not possible in a global study. As a result, the T cell assessments that have been done on COVID vaccine studies to date have been done by special labs for a small fraction of participants in the vaccine studies.
But we are in a new age of medicine. The tools exist today to measure T-cell response quickly, at scale and cost efficiently. We now have molecular assays that can assess the T cell response using DNA from blood that is compatible with almost any sample handling and shipping protocols.
It’s time to start using them.
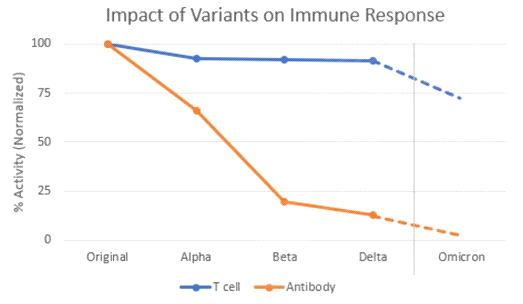
Unfortunately, we are now sitting on the edge of efficacy with the present vaccines. With Omicron, we are seeing neutralizing antibody levels drop to less than 10% of the level seen with previous variants. Even T cell levels, which have held steady in vaccinated people for long past six months, are also starting to drop.
We at Adaptive Biotechnologies, along with colleagues at Stanford University, just published last week that the number of circulating T-cells that can kill Omicron has dipped to about 70 percent of the levels seen against the original strain.
This is predicted by determining which T cell epitopes – parts of the Spike gene that T cells bind – are impacted by the Omicron mutations. For each T cell epitope, we have measured the size of the T cell response. So, we can determine how much of the response is lost due to the mutations.
A third shot of an mRNA vaccine six months after the first round of shots will likely provide a reasonable level of protection. But there is still high risk that the protection will drop even farther with the next variant.
It’s time to rethink vaccine design to take advantage of the T-cell response. If we continue to only focus on neutralizing antibodies as the measurement most predictive of vaccine efficacy, we will wind up with new vaccines designed for mutations that are no longer relevant. We cannot afford to make this mistake.
We need to look at both neutralizing antibodies, and T-cells, to get a more comprehensive view of the breadth and depth of immunity being elicited by new vaccine candidates. We need to take these measurements consistently and longitudinally. We need to know how long the protection is likely to last and we need to make sure that a robust T cell response is induced in everyone.
We – and others – have been raising the alarm about the importance of T cells for the last year and our pleas have fallen on deaf ears. As mentioned above, the T cell response was not practical to measure at scale and neutralizing antibodies for other vaccines served as a good correlate of protection. But we now have better measurement tools and SARS-CoV-2 vaccine efficacy is remaining strong even when antibodies are ineffective. The T cell response must be included at scale in all vaccine studies, and now it’s possible to do so.
This has life and death significance. It is imperative to leverage existing technologies to rigorously study the complete immune response to advance vaccine and drug development, inform public health and guide individual decision-making. Companies like Nykode and Gritstone are working on novel vaccines that consider the breadth of the T cell response. More should be following suit.
The world has changed. We should be nervous. We should be acting immediately to develop vaccines that consider both antibody and T cell responses systemically. The time is now.
November 3, 2021
My Life as a Care Partner: A Perspective by Diane Kennedy
Diane Kennedy
November is National Family Caregivers month, a time to recognize and honor family caregivers for the challenging roles we hold in helping loved ones navigate medical crises. I am honored to share my experience as a care partner, as well as some tips and strategies for coping I’ve learned along the way.
The past four years of my life have been an emotional journey full of ups and downs.
In December of 2017, Todd, my husband of 28 years at the time (now 32 years), began complaining of pain in his back. This triggered an MRI that revealed cancerous lesions up and down his spine. Soon after, he was diagnosed with multiple myeloma, a currently incurable form of blood cancer. At first, I felt overwhelming sadness, which evolved into a strong fear of losing Todd and being alone. After the initial shock subsided, I went into “warrior mode” and put my emotions aside to focus on finding Todd the best possible cancer care.
Todd used to call me his “caretaker,” or “caregiver,” but I never thought those terms truly captured my role in Todd’s cancer battle. We have since landed on the moniker “care partner,” which is a better term for how we work together to become more educated, empowered advocates for Todd’s care.
Care partners like myself often do not have a choice but to go “all in” during the period just after diagnosis. There wasn’t time to do anything other than focus on Todd, his disease, and where to get treatment–but, at the same time, there was pressure to manage all other aspects of life at work and home, including new responsibilities I took on for Todd.
Thankfully, this was just during the initial adjustment phase, and I emerged with strategies and tips to share with anyone on the same journey:
Remember, this process won’t last forever. Have grace for yourself and learn to accept that you can’t do it alone. Others want to help you, communicate what you need – and let them help.
Communicate the changes in your capacity at work and at home as you move through the diagnosis and treatment process. This will reduce stress and give you back some time in the day.
Do something physical. Going for a walk each day helps me be a better care partner! At first, I saw this as self-indulgent, but the physical outlet and fresh air reduces stress, helps me stay positive, and gives me space to process.
Find a support group and talk with other care partners, either in a group or one-on-one setting. It’s comforting, reassuring, and empowering to connect with a community and know that you are not alone. Your doctor or nurse may be able to put you in touch with other care partners, or you can find support through one of the many amazing patient advocacy groups.
Remember that you are ONE member of a robust, expert care team. Find the best doctor and care center available to you, and trust in their guidance. Letting go of the expectation that you need to be an expert is liberating.
Today, Todd is in remission, but we understand that myeloma is a long road. We continue to track his status with regular checkups and minimal residual disease (MRD) testing to monitor his remission and any signs of relapse. We are living our lives to the fullest regardless of the cancer. Last year, we both retired to redirect all our time and energy to advocating for blood cancer patients. Our work as coaches and advocates is incredibly fulfilling.
To all the other care partners out there, I want to let you know that your work does not go unnoticed or unappreciated. Cancer is a long, grueling journey but it doesn’t rob you of your personal power. By taking care of yourself and advocating for yourself and your loved one, you can take back control of your life.
September 28, 2021
Remaining Vigilant Against COVID-19 and Future Pandemics Means Opening Our Eyes to the T-Cell Immune Response
Harlan Robins, PhD, Chief Scientific Officer and Co-founder
This July, I had the pleasure of attending and participating in the second annual Disease Prevention & Control Summit (DPCS) along with Adaptive’s Chief Medical Officer Lance Baldo and Chief Business Development Officer Sharon Benzeno. The summit brought together leaders from global public health agencies, governments, academia, and the biopharma industry to discuss the progress made against COVID-19, next steps in ending the pandemic, and preventing future pandemics. The discussions covered a range of topics including SARS-CoV-2 vaccine development and manufacturing, novel therapeutics, better diagnostics, and the work we need to do now to prepare for future pandemics. As decisions about COVID vaccine boosters loom and concerns about the Delta variant continue, what I heard during the summit seems even more relevant today.
As we have seen since March 2020, combatting pandemics requires speedy collaboration and communication across countries, business sectors, national government agencies and global public health organizations. Meetings like DPCS provide an opportunity for these critical conversations to continue and even for new partnerships to form. As Dr. Jay Butler of the Centers for Disease Control said, “During a crisis is a terrible time to exchange business cards.”
As both a participant and attendee, I came away from DPCS with several ways in which we could both address the current pandemic and prevent future ones.
Reading the Entire Immune Response
To address a challenging problem, we should look at all sources of information that can be part of a solution; understanding the protective response conferred by vaccines from the adaptive immune system requires us to look at both antibody and T cell responses. Studying only the antibody response to vaccines is like reading every other word in a book. You may have an idea of what is going on, but you miss out on the full story. This assessment of T cells and antibodies is needed at every stage of vaccine research and development. It also means incorporating T-cell assessment into regulatory guidelines for vaccine makers to help them incorporate it into trials. As peer-reviewed data mounts, we know that COVID-19 vaccines elicit a T-cell immune response even when antibody levels are low. As we see variants like Delta emerge in the population, understanding the T-cell response becomes even more critical in the long term.
Updating Clinical Trials and Regulatory Guidelines
We don’t understand the complete immune response to this virus. Using antibodies alone as the primary means to measure protection has gotten us far, but it’s indisputable that T cells are another important part of the equation. This has been shown in many peer-reviewed studies, including a recent study published in Immunity by John Wherry and a group out of Penn Medicine. It has also been shown in multiple studies, including a recent study published in Nature, that T cells provide protection against variants, even when levels of neutralizing antibodies are much lower, showing that we need to look beyond this important marker.
Despite this mounting evidence about the role of T cells, many academics, government researchers and pharma companies are not including T-cell metrics in their studies. As a result, this critical component of assessing the adaptive immune response is missing from research. We need support from government agencies on incorporating T-cell response into clinical trials and regulatory guidelines to support the development of SARS-CoV-2 vaccines and therapeutics.
Merging Biology and Technology
This pandemic has made it clear that outsmarting a virus requires harnessing the power of high-performance computing (HPC) and artificial intelligence (AI). For public health organizations such as the Centers for Disease Control, this has meant using AI technologies to improve detection of current infections as well as modeling future spread and emergence of variants.
In pharma and biotech, using HPC and AI can quickly turn massive datasets into actionable insight and therapeutics. Early in the pandemic, we turned to Microsoft Azure to help us tap into the full value of the massive clinical immunomics database generated by our immune medicine platform, including data generated by our COVID-19 research, which we shared with the world through our open public database ImmuneCODE.
As we combat COVID and prepare for future pandemics, we need to continue to combine biology and technology to both understand current outbreaks in real-time and predict the emergence of new diseases.
Remaining Vigilant
The COVID-19 pandemic has shown that if we work together and across industries, we can do what was previously thought to be impossible. To end this pandemic and prevent future pandemics, we need to remain vigilant of both current and emerging viral threats. To develop effective vaccines quickly, we need to fully understand the complete adaptive immune response. This can be done by going beyond traditional ways of measuring immune response, bringing biology and technology together, especially advances in AI/machine learning, and modernizing clinical trials and regulatory guidelines to include advances in measurements of the adaptive immune system.
September 21, 2021
An HQ with a View
Adaptive Corporate Marketing and Communications
The hum of twin engines on Seattle’s Lake Union may interrupt a quiet conversation in the park or a peaceful paddle board past the gently bobbing houseboats. But for Chad and Harlan Robins, brothers and founders of Adaptive Biotechnologies, it’s music to their ears—a welcome reminder of just how far they’ve come.
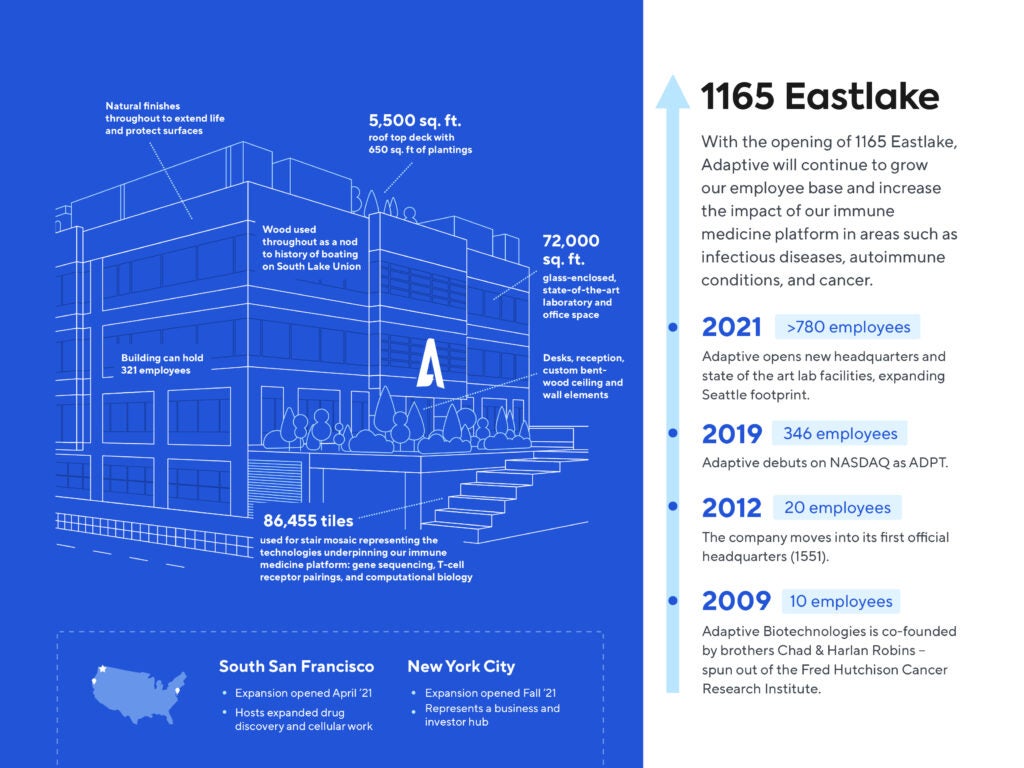
In 2006, Harlan was excited by the biotechnology industry that at the time was just beginning to build momentum in the Emerald City’s South Lake Union neighborhood. With an offer to join the prestigious Fred Hutchinson Cancer Research Center, the scientist looked out over the bustling waterfront scene—seaplanes taking off and landing, schooners passing by with their sails billowing, and the frenetic beauty of what he saw helped seal the deal. Now 15 years later, the visionary company started by Harlan and Chad is an anchor of Seattle’s booming life sciences scene. Adaptive’s growing operations, with a new headquarters at 1165 Eastlake overlooking the lake, is both a reflection of their story and a catalyst, propelling it into the future.
“The science that’s coming out of this city is remarkable, and we’re the beneficiary,” Chad said. “We’re able to hire a lot of talent out of the surrounding institutions and universities, but we’re also recruiting and hiring people from across the country to come to Seattle to make the biotech community and Adaptive even greater.”
Adaptive is ushering in a new diagnostic and therapeutic platform the company calls “Immune Medicine.” Their Immune Medicine Platform combines biology and technology to decode how T cell and B cells, cornerstones of the adaptive immune system, naturally detect, attack and remember disease to create better tests and treatments that may one day help end the patient journey and transform medicine.
With a significant uptick in growth over recent years, it became increasingly clear that the company’s leases at 1551 and 1208 Eastlake could not keep up with its expanding workforce. Recognizing the advantages of staying within the South Lake Union biotech enclave, Adaptive worked with longtime partner and early investor Alexandria Real Estate Equities, Inc. to lock in a location for their new headquarters, a development nestled between Eastlake and Fairview Avenues, just steps away from the Fred Hutch.
“Space is mission critical because it’s the platform where companies like Adaptive do their transformative work,” said Joel Marcus, executive chairman and founder of Alexandria Real Estate Equities, Inc./Alexandria Venture Investments. “Their need for a new headquarters also symbolizes the leadership role that they’ve taken within Seattle’s biotech community and their vision for creating a space that fosters great collaboration and cooperation and for building a first-in-class culture.”
To bring its vision for a new headquarters to life, Adaptive turned to Seattle architect Ben de Rubertis of Flad Architects. An experienced leader in designing for science-based facilities, de Rubertis was inspired by Adaptive’s mission as well as its mandate to create a space expressive of its culture. After months spent talking to a team of executives and getting to know the company, de Rubertis had a plan in place: 72,000 square feet of glass-enclosed state-of-art laboratory and office space to move Adaptive’s science forward and a multitude of unique details and amenities to make sure the company’s culture moves along with it.
“The inspiration for the building design is to really make it easier and more fruitful for Adapters to come in and do their work together,” de Rubertis said. “The idea was to create areas where they can more readily collaborate and see more deeply into their processes and into their science, so that they’re at the top of their performance while they’re at work. We really wanted to create that experience of being in the building where the science is on display.”
Setting the stage
To make Adaptive’s new headquarters stand out as the place to be, de Rubertis designed a 6100-square foot entrance plaza between Eastlake and Fairview Avenues. From Fairview, a monumental stair features colorful, hand-laid mosaic tilework by New York artist Stephen J. Miotto of Miotto Mosaic Art Studios. The installation includes three important Adaptive themes: T-cell receptor pairings, computational biology and gene sequencing. Essentially a walkway connecting Eastlake and Fairview Avenues, the monumental stair was never meant just for Adaptive. In fact, de Rubertis hopes the common area will be a gathering place and source of pride for the entire neighborhood.
“South Lake Union is rapidly developing into a biotech hub,” de Rubertis said. “And we think that this stair really helps to demonstrate what’s special about the science that’s happening here, whether it’s at Seattle Cancer Care Alliance, Fred Hutch, Adaptive or any of the other companies doing amazing work here. It speaks to three languages of biotech coming together in one location.”
Accessible via the plaza, Adaptive’s second-floor lobby features a seating area, a reception desk and a decorative partition made up of 3-D trapezoids and triangles. The motif, referenced first on the monumental stair and carried throughout the building, represents a T-cell receptor pairing, one of the key scientific concepts that informs the adaptive immune system.
Past a set of see-through security turnstiles, a lounge space will feature more mosaic tilework by Miotto Mosaic Art Studios and floor-to-ceiling windows along Fairview that face out toward Lake Union. De Rubertis used the proximity to the water and the neighboring Center for Wooden Boats as inspiration for design elements like a muted blue-gray palette and gently curved wood slats along the wall and covering a portion of the ceiling, all of which nod to the area’s unique boating-building past.
Spotlighting science
If the second-floor common spaces set the stage, on the third level, science steals the show. With an elevator bank and interior stairwell in the center, a ribbon of connected glass-enclosed laboratory space lines the outer walls, allowing both natural light and sense of camaraderie to flow through from one side of the building to the other.
“Highlighting Adaptive’s science is absolutely essential to the building design,” de Rubertis said. “From the moment you emerge from the stairwell or elevator bank onto the third floor, you’re introduced to the science. You’re being told a story. Storymaking is also a really important part of building experience and culture-making at Adaptive, so the chance for us to pack those two essential ideas into the design was really the key opportunity here.”
Just as the transparent and continuous lab space beckons Adaptive scientists to connect with each other and colleagues who are working on different parts of the process, alcoves—dubbed “science parlors”—located opposite the central stairwell and tucked at various points along the ribbon wall offer intimate spaces for more collaboration. The parlors vary in size and feature lounge-like seating and whiteboards for breakout learning sessions in full view of the work that is being done at Adaptive.
Other unique details continue the culture-making experience on the third floor. For example, employees can fuel up on coffee, cold beverages and snacks at the centrally located refreshments station. Meanwhile, a mural being developed by local artist Katy Stone will offer a splash of color to a sundrenched but otherwise stark white wall that continues up to the fourth floor directly under a skylight.
Centering culture
On the fourth floor, de Rubertis set out to use every square inch of space available to help the Adaptive culture thrive. Executive offices, banks of low-profile desks and conference rooms fill the interior space, while a glass bifold door opens to an outdoor terrace that stretches the length of the building’s north side. Boasting tables, lounge seating and a living roof garden, the terrace is the perfect place for Adaptive employees to work together, let loose or just enjoy fresh air and a great view.
While the well-appointed outdoor space stresses Adaptive’s synergistic connection to Seattle and the active lifestyle its geography inspires, de Rubertis designed several indoor features to reflect that same sentiment. A glass-enclosed central stairwell runs the vertical length of the building with openings on levels two through four. To encourage employees to take the steps, de Rubertis widened the stairwell and commissioned local metal fabricator Architectural Elements to create the custom laser-cut metal guardrails. A skylight provides natural light from above and a light strip tucked along the wall lends architectural illumination and warmth. At street level on the west-facing Fairview Avenue side of the building, workers traveling by foot, bicycle or even kayak can take advantage of showers and changing rooms before heading up to work.
With its abundance of science and people-centric spaces, Adaptive’s new headquarters positions the company for its next chapter of growth.
”Our biggest asset, by far, is our people,” said Robins. “The culture that we’ve created provides an environment that lets people be creative and flourish. That is pretty special.”