Adaptive President Julie Rubinstein Reflects on World Cancer Day
Julie Rubinstein, President
Eighteen years ago, I began a journey with my dad that profoundly impacted me personally and professionally. At the time, I was expecting my oldest daughter Emily when my healthy and active father was diagnosed with a rare and then hard-to-treat bone marrow disorder called myelofibrosis.
With limited treatment options, this diagnosis did not have a great prognosis. Through the incredible organization Gift of Life, my dad was twice matched with selfless bone marrow donors, enabling him to undergo two separate life-saving stem cell transplants. Five years ago, thanks to scientific advances, I was able to be his donor for a third transplant.
During that time, I experienced first-hand that we could save lives by looking within ourselves. For hundreds of millions of years, the body’s immune system has been evolving to better protect us and keep us healthy. It’s a force inside your body so powerful that most of the time, it’s able to detect and fight disease —often before you even realize that you’re sick. Our body’s capability is nothing short of amazing.
At Adaptive Biotechnologies, we believe that we have a great opportunity to harness this capability to power a new era of medicine – which we call immune medicine – to detect and treat disease by learning from the way the body’s immune system does it naturally. Many of the clinical products we have developed are using our technology to help people with certain leukemias and lymphomas detect the smallest amount of remaining blood cancer cells that can stay in the body during and after treatment or transplant –a sign that the cancer is returning.
We are also working in partnership with Genentech to leverage our immune medicine platform to identify T-cell receptors – the first responders of your adaptive immune system to recognize cancer – that can be engineered into cellular therapies for cancer patients. The progress in this area has been amazing and life changing for so many people in need of new treatment options.
On this World Cancer Day, I am in awe of the cancer community and the resiliency that has been shown during this especially difficult time. Patients are still fighting. Caregivers continue to show up. Physicians are seeing their patients. Donors are still raising money. Research advances. At Adaptive, our lab and lab support staff have continued to show up every day, despite their own personal hardships caused by this pandemic.
The power of the human body to fight disease is nothing short of extraordinary and the individual stories behind every immune system are unique. By decoding these stories, we can create better endings for more people battling disease, whether it’s cancer, COVID-19, or beyond.
Today, at the young age of 78, my dad is cured. As a long-time volunteer and board member for The Valerie Fund, I’ve had a front seat to witness the incredible therapeutic advances that are leading to more cures in children with cancer and blood disorders. At Adaptive, we will continue to innovate to give everyone this same chance.
February 3, 2021
Learnings from the COVID-19 Immune Response Will Accelerate Healthcare Innovation
Lance Baldo, Chief Medical Officer
It has been about one year since SARS-CoV-2 hit the U.S. and, in that time, there have been over 100M reported cases and over 2M deaths globally. As the world races to develop solutions, including therapies and vaccines, our greatest defense has been our own immune systems. We have gained a tremendous amount of knowledge by studying, with speed and scale, how the immune system responds to the virus – not just on an individual level, but across the population. This knowledge is informing the answers to some of our most pressing questions, including:
Why do some people get severely ill, and even die, while many people experience mild symptoms or no symptoms at all?
Is someone who has been infected with this virus “immune,” and for how long?
How long will vaccines last and how will they work against emerging strains?
At the recent Precision Medicine World Conference, experts from around the globe gathered virtually to share insights gleaned over the past year from the lab, clinic, and bedsides of those battling COVID-19. In a panel moderated by Dr. Andrew von Eschenbach, president of Samaritan Health and former commissioner of the FDA, I had the opportunity to participate along with esteemed colleagues Catherine Blish, Akiko Iwasaki, and Mathai Mammen to address these questions and more, including how these learnings might affect the future of medicine.
The bottom line – our learnings thus far will impact not only our ongoing response to new variants of this virus, but they will also shape the way we approach treating a whole spectrum of diseases moving forward. Read on for key highlights from this discussion.
Takeaway #1:The seed and the soil
While we are getting better at identifying correlates of disease severity with COVID-19, it remains difficult to predict how an individual may or may not respond to infection. Certain patients experience a mild illness or no symptoms at all while others are catapulted into respiratory, cardiac or other organ distress with potential dire and even long-term sequalae. As Andy so eloquently framed the conundrum: it’s not just the seed that matters, but also the soil. How the virus takes hold is highly dependent on the host and how and when their own immune system responds.
There are many factors contributing to such diversity of response. For starters, there is a tremendous amount of variability in the early innate response to the virus that kickstarts the broader immune system’s defense. Studies have found that the virus has been able to evade innate immune recognition and early type 1 interferon response in people who get severe COVID. This can lead to other types of hyper-inflammatory reactions that are less adapted to fighting this virus and ultimately end up harming patients instead of helping. Co-morbidities also play a major role and may hasten these hyper immune responses.
The work we are doing at Adaptive to decode the T-cell response to COVID-19 has shown that the adaptive immune system demonstrates a range of response to infection. For instance, in some patients who get really sick, there can be a blunting of the T-cell signal. For those in whom the T-cell signal returns, they tend to recover, but in those in whom it does not return, they tend to do much worse. It is not known whether this is causative or associative, but this underscores the pivotal protective capacity of T cells and the potential clinical utility in determining prognosis. If we can figure out who is having which response and why, this information will help inform how we manage and treat disease.
Takeaway #2: Mind your B’s and T’s
Now that we have multiple vaccine options available to the public, we face a new question – how long are we protected? While we have typically looked to antibodies to help inform this question, we have learned that we also need to look at the T cells to fully understand the immune response. Specifically, does a person have T cells that are specific to this virus, and from which part of the virus is a T-cell response being induced? This is critical information for vaccine developers in the planning and rational design of future vaccines and boosters.
Early on, the spike protein of the coronavirus received the most attention from vaccine developers, understandably, given the historical appreciation of the importance of this viral component to replication and the need to move quickly. Many experts have noted that since only a portion of the total T-cell response is spike protein-derived in a native response to infection, future and continued development of vaccines should optimize for the immune response induced by binding antibodies, neutralizing antibodies and T cells, focusing on the breadth and depth of the response. Breadth is likely to be very important for long-term durability and effectiveness, especially with new and emerging variants. Adaptive is beginning to address this consideration by analyzing blood samples from those who have had infection with the new strains compared to earlier, dominant strains of SARS-CoV-2. As we learn more about the immune response to vaccines and primary infection it is certain that T cells will continue to play a key role in this new phase of understanding and controlling this pandemic.
Takeaway #3: Precision medicine is here to stay.
As we’ve seen in other disease areas such as cancer, immune profiling may dictate which therapeutic is appropriate for an individual person. This specific level of information can alter the course of a disease. Beyond oncology, we are learning how our immune systems respond to a whole spectrum of diseases. COVID-19 has accelerated our research and understanding of the synergies between therapeutics and the populations they aim to serve. Simply put, there is ‘no one size fits all’ when it comes to addressing most diseases.
Takeaway #4: Prepare for the long haul.
As in many other disease areas, getting over the initial illness doesn’t necessarily mean you are out of the woods. This is becoming increasingly evident with the tens of thousands of people – often referred to as “long haulers” – who are now experiencing symptoms months after the onset of COVID-19. Published studies and the largest grassroots patient advocacy group, Survivor Corps, have uncovered nearly 100 symptoms reported even after tests no longer detect the virus, including muscle fatigue, shortness of breath, and cardiovascular problems. This is an important area for continued research, and one that Adaptive is already studying to better understand the role of the T cell in long COVID. The other public health piece of this – and it is a significant one – is organizing post-care facilities that address these long-term consequences.
Takeaway #5: We have begun an era ofunprecedented collaboration – let’s keep it up.
The most heartening part of this past year is watching the science and public health communities come together to accelerate innovation. We’ve leaned into the lessons from other public health crises – HIV, cancer and other diseases – and what we’re learning, and sharing about the immune response to this virus is certain to have applications far beyond this pandemic and into the next generation of therapeutics. We can all agree that we must remain in this, together.
January 6, 2021
Powering the Age of Immune Medicine
Chad Robins, Chief Executive Officer & Co-founder
Ten years ago, my brother Harlan and I started Adaptive Biotechnologies on the premise that if we could read the genetic language that tells us how the adaptive immune system detects and treats disease, we could apply these natural abilities to improve outcomes for patients.
Our body’s capability is nothing short of amazing, and we fundamentally believe that there is no greater opportunity for medicine than to use this inherent capacity to find, treat, and maybe even cure many different diseases.
Our global understanding of the immune system has grown significantly over the last decade. We have seen the critical importance of understanding immune response unfolding on a global scale as the scientific community has come together to fight the novel coronavirus.
Just as our immune systems have evolved, so has Adaptive. Over the past decade, we built our proprietary immune medicine platform, unlocking the incredible potential of the adaptive immune system inside each one of us. We have expanded from propelling research to launching first-in-kind clinical diagnostics, to developing new classes of therapeutics.
Today, we take another step in the evolution of our company – a new brand identity, and a new symbol: The Adaptive A.
The Adaptive A symbolizes the immune system and its evolution over time, how each person’s is unique, and the variations within each of us. It is a window into the stories that each immune system has to tell, and a celebration of diversity, and a symbol that captures the promise of a new chapter in the diagnosis and treatment of disease.
We envision a future where all that we can learn about how the adaptive immune system naturally diagnoses and treats diseases can be incorporated into the routine clinical practice; once we establish a therapeutic or diagnostic for one disease, we can do it again and again.
The Adaptive A captures the complexity of our immune systems and the promise of a new chapter in the diagnosis and treatment of infectious disease, cancer, autoimmune conditions and more.
At Adaptive, we remain uniquely positioned in our own category as we propel a shift in disease management with the goal of improving lives everywhere. We are thrilled to ring in the new year with a new symbol that reflects the evolution of our company and all of the possibilities that lie ahead.
Welcome to the Age of Immune Medicine. Powered by Adaptive.
– Chad
December 8, 2020
New Minimal Residual Disease (MRD) Research is Great News for Blood Cancer Patients
Lance Baldo, Chief Medical Officer
Until about 25 years ago, treating people with HIV was difficult and uncertain—and the disease itself was practically a death sentence. Improved diagnostics and technology that could detect viral load guided newer therapies and HIV became a treatable disease. A similar paradigm has occurred in blood cancer; the advent of monitoring minimal residual disease (MRD) to guide innovative therapeutics is changing this area of medicine. The ability to assess depth of remission is providing physicians with a more accurate and reliable way to manage therapy and improve outcomes.
The real-world impact of the use of Adaptive’s clonoSEQ® Assay is exciting for physicians and patients alike. It is the first and only FDA-cleared test that measures MRD in select blood cancers including multiple myeloma, chronic lymphocytic leukemia (CLL) and B-cell acute lymphoblastic leukemia (ALL). With proper input material it can find one residual cancer cell amongst a million healthy cells.
The ongoing generation of evidence is critical to advancing the clinical adoption of MRD testing, and we recently shared a significant amount of new research at the American Society of Hematology (ASH) 2020 conference. The bottom line from the more than 45 abstracts including clonoSEQ data being discussed at the meeting is this: when clinicians use precise MRD assessment to make treatment decisions, patient outcomes get better and overall costs go down.
Why is that? When doctors are able to get more specific and accurate information about a patient’s disease status or how that patient is responding to treatment, they can have more robust conversations with the patient about treatment goals, treatment effectiveness and future prognosis. Those conversations, combined with the insights provided by the MRD results, enable clinicians to better tailor their management approach to achieve the most optimal outcome for the patient. Put simply, this puts patients and their providers in the driver’s seat when it comes to managing their disease.
The advancements clonoSEQ is bringing to the table today are indeed comparable to viral load testing for HIV, which was introduced in the 1990s and is now standard of care. The ability to measure and track disease load validated paradigm-shifting therapies in a way that had never been done before. This has become increasingly true for hematology as well.
Data presented at ASH this year adds measurably to the ever-growing body of evidence validating MRD as a critical measure of outcomes in patients with blood cancers. This has become especially important as novel drugs are making deeper responses and longer-lasting remissions possible for more and more blood cancer patients. Clinicians are and should be using MRD results to help make sense of their options and how to best deploy them.
As with all developments in medical science, we still have much to learn. How can MRD testing advance the ways we have traditionally monitored certain cancers? One example is imaging, which can be expensive and lacking in specificity while also exposing patients to radiation. Any developments that could reduce the need for imaging would be important for physicians, patients and the overall healthcare system. In certain B-cell lymphomas, early evidence suggests that MRD may be able to deliver on this promise, whether by replacing the need for imaging in some settings or by empowering a strategy of “MRD-guided imaging” in others.
For a clinician like me, it is really encouraging to see that patients are seeing the benefits of MRD testing not only in clinical trials, but also in current clinical practice. Patients do not want to wait, nor should they, for a highly precise diagnostic tool that gives them greater potential for successful treatment – and a fuller life.
December 1, 2020
T Cell Testing Outperforms Antibody Testing in Determining Prior COVID-19 Infection
Harlan Robins, PhD, Chief Scientific Officer and Co-founder
COVID-19 rates are at an all-time high. With no singular containment strategy underway in the U.S., it has become more critical than ever to understand who has previously been infected by the virus, whether or not they displayed symptoms. Traditional serology tests can detect the presence of antibodies in the blood, indicating that the body has responded to an infection in the past, but antibodies appear to wane over time. Moreover, recent studies show that some people never mount a detectable antibody response and are instead able to fight off the infection with other immune cells, T cells, before antibodies even appear. Having different tests to help detect recent or past infection is critical to gaining a more accurate understanding of immunity on a population-wide scale.
As part of our ongoing effort with Microsoft to build the TCR-Antigen Map and develop novel, more accurate diagnostics to diagnose many different diseases, we’ve analyzed over 1,500 SARS-CoV-2 samples to date in the ImmuneCODE study. Our most recent study published on the preprint server medRxiv shows that Adaptive’s T-cell test under development outperformed commercial EUA approved antibody testing as an indicator of past SARS-CoV-2 infection, with 99.8% specificity. These data support the launch of T-Detect™ COVID, which will be available later this fall. The study also found that T-cell response differed and was considerably higher in individuals with greater disease severity, whereas there was no correlation between disease severity and antibody levels in these recovered patients. Taken together, these data add to the growing body of evidence that T cells are critical in understanding our immunity to the novel coronavirus.
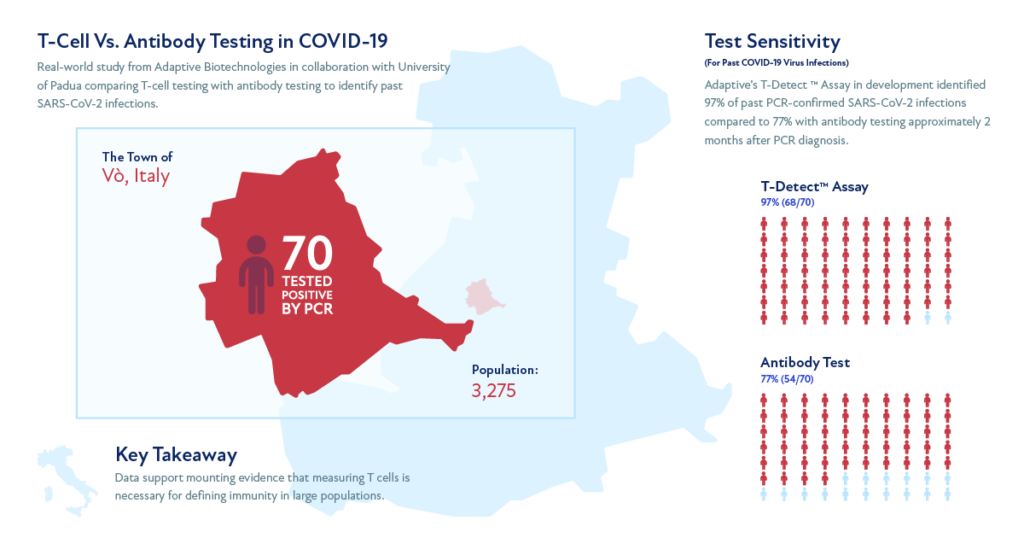
Vo’, Italy – One Town’s Mission to Contain the Pandemic
On February 21, 78-year-old Adriano Trevisan was the first person in Italy to die of pneumonia due to COVID-19. He was from a small town in northern Italy called Vo’, a one-hour drive west of Venice. Two days following his death, the entire municipality of Vo’ was placed under a strict lockdown and almost immediately, an aggressive testing campaign was initiated. At the beginning and end of a 14-day lockdown, 2,900 residents – 97% of Vo’s population – were tested using PCR to confirm the presence of the virus. More than 40% of those who tested positive showed no symptoms, and this study was one of the first showing that these asymptomatic cases were key to the undetected spread of the virus. Those who tested positive were either quarantined at home or, in severe cases, hospitalized. All residents were encouraged to limit their movement outside of their homes. By March 23, the spread of the illness had stopped and there were no new infections. These data were published in Nature and were widely cited because they provided real world evidence for how the pandemic could be controlled through proper testing and quarantine of affected individuals.
A Breakthrough in Detecting Past SARS-CoV-2 Infection and a Potential Key to Immunity
Vo’ is one of the only locations in the world where previous SARS-CoV-2 infection status is “known” for an entire population. It is thus ideal for understanding how to measure past infection. Two months after the initial lockdown, Adaptive collaborated with University of Padua and Ospedale San Raffaele in Milan in a follow-up study of 2,290 residents, including 70 people who had tested positive with PCR testing on initial analysis. Study participants underwent antibody testing with a EUA approved commercial test (IgG) and T-cell testing with Adaptive’s T-Detect. T-Detect identified 97% of past infections, while antibody testing identified only 77%. Additionally, the T-cell response was higher in symptomatic versus asymptomatic subjects, demonstrating a relationship between disease severity and the amount of detectable T cells, whereas antibody levels did not correlate with disease severity in this recovery period.
Notably, of the 2,200 people who originally tested negative for the virus using PCR¬, 45 tested positive for virus-specific T cells with T-Detect. About half of them had reported symptoms, either before or after PCR testing, or had household exposure. Therefore, T-Detect may also identify past infections that had been missed by prior PCR testing.
Assessing Protection from Future Infection
As infection rates continue to soar, T-cell testing can help us understand the true prevalence of COVID-19 in our communities as well as the degree to which our population is protected from future infection. At the individual level, the availability of a T-cell based clinical test could be useful for people who suspect they may have had COVID-19, but were either unable to get tested or had a negative PCR test at the time of their illness, and who want to know for sure whether they had the disease.
While there is still much to be learned about immunity to and protection from this virus, emerging data show that antibody protection may be transient, and T cells could be the key to durability of protection. Such insights will be critical as we progress toward lasting solutions for the COVID-19 pandemic, including the race toward a vaccine.
The coronavirus pandemic has thrust testing into the spotlight, highlighted by long lines to get tested across the country. We know that accurate, sensitive, and timely diagnosis is paramount in fighting and containing this virus. The same can be said for many diseases; having the right test goes beyond COVID-19.
Today, in parallel with our efforts to bring forth a novel T-cell-based test for COVID-19 to market soon, another major focus at Adaptive and for those in the oncology community is the ability to test for “minimal residual disease,” or MRD. MRD refers to the small number of cancer cells that can stay in the body during and after treatment. Often, these cells are present at such low levels that they do not cause any physical signs or symptoms. However, they may be a signal that cancer is returning, and their absence can be a signal that the disease is under control.
As one of the strongest predictors of patient outcomes in blood cancer, it is no surprise that more and more oncology and hematology treatment developers are integrating MRD tests into their clinical trials. In fact, we recently entered into a collaboration with GlaxoSmithKline (GSK) to use our clonoSEQ® Assay – the first and only FDA-cleared in vitro diagnostic for MRD monitoring in patients with chronic lymphocytic leukemia (CLL), multiple myeloma (MM), and B-cell acute lymphoblastic leukemia (ALL) – across GSK’s hematology and oncology portfolio. This adds to a number of partnerships already established with AbbVie, Amgen and Genentech which incorporate clonoSEQ into their blood cancer clinical trials.
Not only is the use of MRD testing growing in clinical trials, but it is also becoming more routine in the post-approval patient journey. MRD status can help patients and doctors understand how the body is responding to treatment and make timely course-corrections as needed. Especially today, as novel therapies drive better response, MRD testing is increasingly important to assess the depth and durability of that response, so clinicians are prepared to intervene quickly and patients have the opportunity to make choices and plan.
As MRD testing continues to become more commonplace, we’ve recently launched a study with the primary goal of understanding why and how MRD testing is used in patients with ALL, CLL, MM and Non-Hodgkin’s Lymphoma (NHL) to identify trends and best practices for the broader oncology community. As part of our new WATCH registry, we will be following patients’ MRD data and treatment changes for up to three years to understand how MRD testing with clonoSEQ is used, what decisions physicians are making based on MRD results, and qualitatively, the correlation between MRD and patient outcomes.
Knowing MRD status – with a test that, given sufficient sample input, can detect one cancer cell among a million cells – gives patients and doctors the confidence and empowerment they need to stay in the driver’s seat of their disease. In the coming weeks, there will be a lot of new data shared about innovation in both testing and treatment at the American Society of Hematology meeting. I look forward to sharing some thoughts around those advances soon.
Testing is a backbone of treatment. As oncology treatments continue to advance and become more personalized, and the options continue to widen, so too should our focus on diagnostics to ensure physicians have the best information to make the best decisions for their patients.
September 18, 2020
The Case for T-cells: Understanding Exposure and Immunity to COVID-19
Harlan Robins, PhD, Chief Scientific Officer and Co-founder
In light of the COVID-19 pandemic, understanding the role of the immune system has become critical in deciphering how this highly contagious virus affects people across the globe of all ages, ethnic backgrounds, and social backgrounds, with widely varying responses. This has unequivocally brought the role of the immune system to the forefront of research and the public discussion, making Adaptive’s immune medicine platform more relevant than ever. We are seeing that with this virus, as with many other pathogens, the T cell provides a key link to understanding exposure and immunity when it comes to COVID-19. Now we have the ability to use T cells to detect SARS-CoV-2 and leverage this capability to measure and monitor a more comprehensive immune response to vaccines in development.
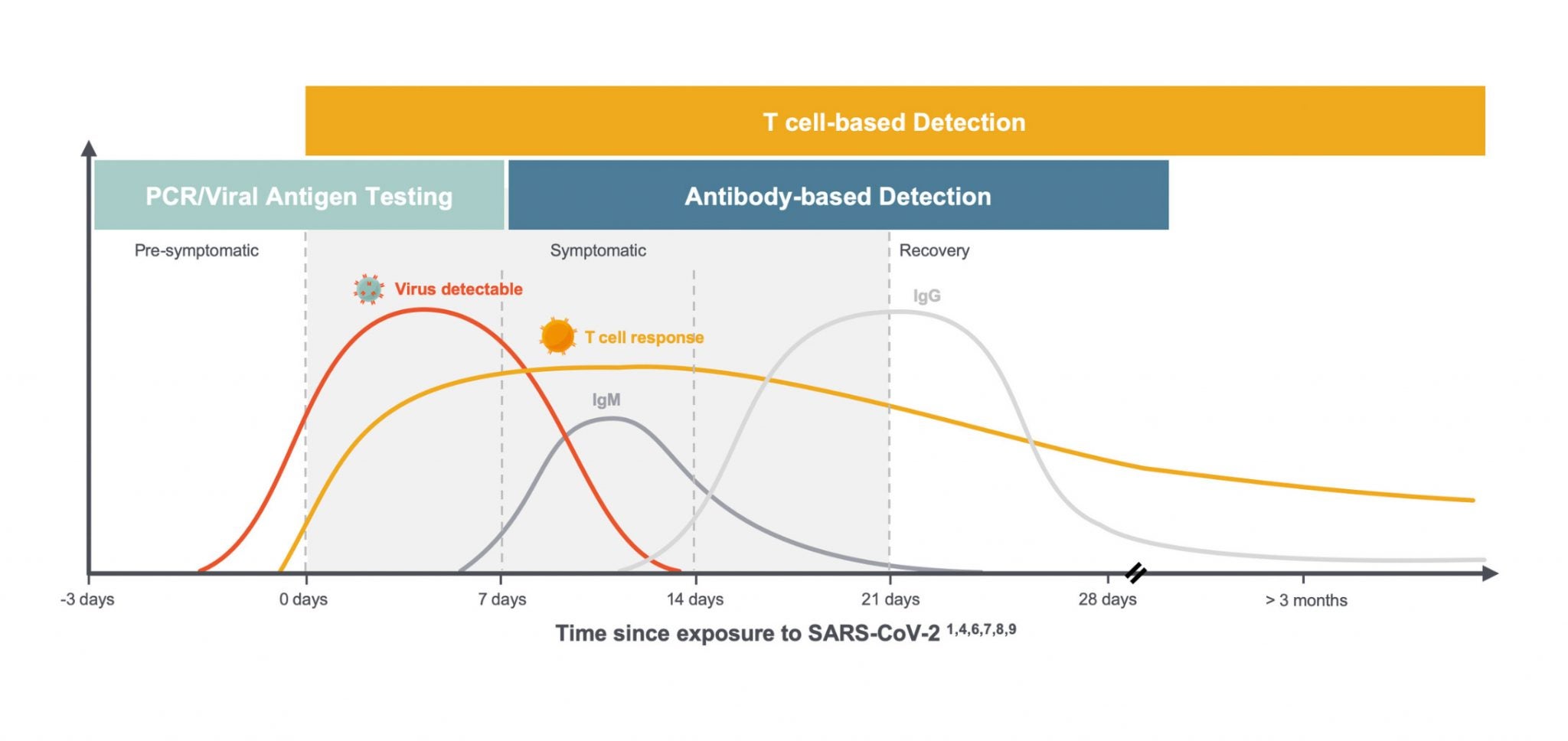
Critical role of the T cell in the immune response to SARS-CoV-2 We and others are learning a great deal about the critical role T cells play in the immune response to SARS-CoV-2. Specifically, exposure to the novel coronavirus can induce virus-specific T-cell responses without inducing antibodies and can be detected up to 100 days after symptom onset, the maximum time period currently available to assess response,1 as shown in this diagram below.
Much of what we are learning about T cells is consistent with what we see in the immune response to other viruses, but the combination of global scientific focus and the number of people infected with the virus in such a short period of time has led to an understanding of the variability of individual responses on a greater scale. In the setting of COVID-19, we are seeing:
T-cell responses arise earlier than antibodies and last through clearance into convalescence. 2
T cells play a critical role in supporting the development of antibodies by B cells and can serve as the first signs of an immune response to SARS-CoV-2 infection. 3
The majority of COVID-19 patients generate a T-cell response comprised of both CD8+ T cells, or “killer” T cells which destroy virus-infected cells, and CD4+ “helper” T cells, which help other immune cells, including B cells which produce antibodies. 5
CD8+ & CD4+ T cells were observed in convalescent patients with mild and severe COVID-19 disease. 6
Solving a big data problem to study the T cell – the critical missing link in immunity
What makes the task seem daunting is that T cells have been historically notoriously hard to study. Our bodies have hundreds of millions of different T cells in order to be prepared to respond to millions of different types of threats. Most researchers have continued to rely on techniques to either measure the immune response solely based on antibody levels, or sometimes measuring T cells using techniques that are expensive, bespoke and low throughput.
At Adaptive, we set out to solve this problem several years ago. Our platform enables us to identify the specific T cells that map to any disease quantitatively at unprecedented scale, speed and precision. Soon after the pandemic hit, our team at Adaptive Biotechnologies, along with our partners at Microsoft, worked quickly to map the T-cell response to SARS-CoV-2 across the population to make these data freely available via ImmuneCODE, which we believe to be the largest database for the T-cell immune response to this virus.
To date, we have analyzed over 1,400 de-identified patient samples. From these samples, we have identified over 135,000 T-cell receptors (TCRs) that map not only to the spike protein but to 10 other specific parts of the virus which we have shown to be most likely to induce an immune response. It is our hope that these data will help researchers around the world in their quest for solutions to this pandemic.
In addition to making these data publicly available, we have developed two applications: a T-cell based diagnostic, and a T-cell monitoring tool for vaccine developers.
Benefits of using T cells to detect SARS-CoV-2
Using a set of identified “shared” TCRs that are seen across multiple infected individuals, we identified a T-cell signature that can be used for diagnostic purposes. Data from Adaptive Biotechnologies and from others to date show that the properties of T cells, outlined above, could make a test that detects virus-specific T cells a more effective way to assess SARS-CoV-2 exposure before antibodies arise and after they wane.
Comparing T-cell signature with antibody serology
To demonstrate this, we recently conducted a head-to-head study in a real-world setting comparing our test under development with two leading serology tests in 100 patients, ranging from active infection through convalescence. The tests were set at 99.8% specificity to minimize false positives. In this study, 94% of patients were detected as positive by Adaptive’s T-cell test under development vs. 90% (IgG and IgM) and 87% (IgG only) for the serology tests, respectively.1
What we are learning about immune response to this virus from our own studies and other research highlight three reasons that may explain the higher sensitivity of a T-cell test:
Patients could be tested after the T-cell response begins but prior to seroconversion. Two of the participants who originally enrolled in our ImmuneRACE study as “exposed” subjects became acutely infected prior to sample collection tested positive for T cells but not for antibodies.
Some patients may effectively fight the virus with T cells alone and never seroconvert. One T-cell positive patient in our 100 sample cohort was asymptomatic with two positive PCR tests, but tested negative by both antibody tests. Other researchers have also reported infections that lead to T-cell response but no detectable antibody response.4
Antibodies wane over time. In our data, we have seen persistence of T cells for most patients as far out as we have measured (~100 days). Other studies have demonstrated that, in contrast, antibodies seem to wane over time although we have not yet observed this in our own data. Literature shows in another coronavirus infection, SARS-CoV-1, that virus specific T cells have been routinely detected in studies in the years following the initial SARS outbreak, including at least a decade after initial infection, while antibodies waned quickly. 10,11
These results, together with a growing body of evidence indicating T cells can be present in the absence of antibodies, suggest the potential utility of Adaptive’s T-cell based approach to detect immune response to SARS-CoV-2 earlier, and in less severe cases, than tests that detect antibody response.
Regulatory submission
Detection of recent or past infection is our first application, and we are currently working with the FDA to generate and package the data required to submit for Emergency Use Authorization (EUA). We anticipate that the data we continue to generate will expand the clinical applications for our T-cell based testing approach to potentially include assessing pre-existing immunity based on cross-reactive T cells, post infection immunity, and immunity from a vaccine, which may need to be monitored for possible boosters over time.
The need to study T cells when measuring and monitoring immune response to vaccines
As we learn more about the role T cells play in immunity, vaccine developers are recognizing the need to measure the T-cell response in addition to the antibody response to their vaccines. The same qualities that make a T-cell test ideal for diagnostic purposes also underscore its utility for measuring immune response to vaccines. We recently launched immunoSEQ® T-MAP™ COVID as a tool to offer vaccine developers a way to integrate our map of SARS-CoV-2-specific T cells into their vaccine trials.
This is the first molecular T-cell monitoring tool for SARS-CoV-2 that accurately, quantitatively, and reproducibly measures the T-cell immune response to vaccines and tracks the persistence of that response over time. We are providing data that map those TCRs to SARS-CoV-2 antigens, a capability that may significantly improve the ability to measure the immune response to vaccines in development. Importantly, we can do this from a simple blood sample that does not require any special storage or handling.
Speed and samples are needed to learn more
Globally, we are all moving quickly to learn more about the virus and find solutions that will help us turn the corner in this fight. We believe that T cells are key to understanding exposure and immunity – one of the many important pieces of this very big puzzle. Our focus remains clear. We will continue to map T cells at scale, track their immune response to vaccines in development, and track their persistence over time, working together in this collective cause to help end this pandemic. If you are interested in contributing to this important effort: Institutions or collaborators interested in contributing blood samples can direct inquiries to COVID19ImmuneResponse@adaptivebiotech.com, and our ImmuneRACE study is still recruiting – visit www.ImmuneRACE.com for more information.
Snyder, et al MedRxiv preprint, 2020
Funk, et al. Frontiers in Pharmacology, 2020
Sekine, et al. BioRxiv preprint, 2020
Gallais, et al. MedRxiv preprint, 2020
Grifoni, et al. Cell, 2020
Peng, et al. BioRxiv preprint, 2020
Paolo, et al. Pediatric Allergy & Immunology, 2020
Subbarao, et al. Immunity, 2020
Channappanavar, et al. Immunol Res, 2014
Tang et al, J Immunol, 2011
Ng et al, Vaccine, 2016
September 1, 2020
How Blending Novel Technologies, Big Data and Bright Minds Are Cracking the Code on COVID-19
Julie Rubinstein, President
Earlier in my career, in the late 90s and early 2000s, I had the opportunity to work in the “global e-business” groups at two large pharmaceutical companies. At that time, e-business was a new noun – a word widely used across industries but with so many different and emerging meanings. In healthcare, e-business was the start of a new era of data collection and information delivery across the industry.
Nine months ago, my peers and I marveled at how far we’ve come in 20 years with the convergence of biotech and tech, the genomic revolution, the way in which data is helping segment patient populations for more targeted therapies, and the emergence of machine learning to advance research and discovery in healthcare. “E-business” is no longer a noun used anywhere, but it is very much part of everything we do in business and in healthcare.
We are now in the midst of another transformation of the use of big data in healthcare. Collaborative efforts throughout the industry, often propelled by technology like AI, have accelerated our ability to obtain information about the biology of the SARS-CoV-2 virus and how people across the globe are responding to it. This is fundamentally altering the way therapeutics and vaccines are researched and developed – in record time – so that patients can get the care they need.
At Adaptive, we are focused on how people across the globe are responding to the virus. By decoding the adaptive immune response at the individual and population level, we aim to make sense of the interaction between the virus and the human body from exposure to infection to recovery. This is a very hard but solvable big data problem if you have the right technology and the right minds behind it.
In 2018, Microsoft and Adaptive forged a partnership to bring together MSFT’s machine learning, AI and cloud computing to our immune medicine platform – accelerating our ability to map the trillions of T-cell receptors to the millions of clinically-relevant disease antigens to which they bind. As my colleague, and partner, Peter Lee at Microsoft, once said, “the adaptive immune system presents an extremely large but beautiful machine learning problem.”
Why? Because our immune cells have evolved to be massively diverse and dynamic to protect us from millions of different signals of disease that our bodies encounter every day. And each person’s immune system is different, which is why people are reacting so differently to this novel coronavirus. Every single person presents the virus a little bit differently to their own immune system, and we have evolved this way as humans to ensure that no virus or germ can completely eradicate the human race.
Since the immune system sees SARS-CoV-2 just like it would any other virus, we were able to quickly mobilize our platform to map the T cell response across thousands of people from around the world. All of the T cell response data that we’ve collected so far is being made freely available to the scientific and public health communities to help accelerate solutions.
At the same time that we have been generating and releasing this T cell mapping data, researchers around the world have been publishing studies showing that antibodies don’t tell the whole story about the immune response to the virus. We now have the ability to broaden the definition of immune response to include the T cell response at scale to inform more accurate and effective diagnostics, therapeutics and vaccines.
The pandemic has spurred many novel partnerships and innovations to expedite and make drug discovery more efficient, breaking down barriers as we band together as an industry to advance solutions as fast as technology can glean new data. Take for instance, the global COVID R&D Alliance that is bringing together 20 of the most experienced life science and drug development companies – like Schrödinger, Amgen, Pfizer and others – to identify, study, and accelerate promising treatments for COVID-19. Recently, Google Cloud joined this alliance, donating over 16 million hours of high-computing technology to advance solutions.
Thanks to AI and other novel technologies, today we can harness data to crack the code of disease and the immune response to disease in ways unimaginable, until now. As data continues to emerge at an unprecedented rate about the SARS-CoV-2 virus and the immune response, it’s clear that there is no one-size-fits-all approach. Only by blending the best minds with the best of science and tech can we continue to make a true difference in how this and future pandemics are defeated.
August 6, 2020
Senior Vice President Charles Sang on Expanded FDA Clearance of clonoSEQ® in CLL
Charles Sang, Senior Vice President (Retired)
I’ve known far too many people who have received a cancer diagnosis, navigated the initial shock, and bravely taken on all of the ‘stuff’ that comes with it – finding the right clinician, deciding on a treatment plan, and readjusting their life to the unknown.
What if my treatment stops working? What happens if my cancer returns? How long will I stay in remission?
Treatment for blood cancers has evolved rapidly, and the measure of minimal residual disease, or MRD, is becoming an increasingly important measure of the presence of cancer throughout the treatment journey. And now, patients living with the most common type of leukemia – chronic lymphocytic leukemia, or CLL – have a new way to get answers to those common questions that often keep them and their loved ones awake at night.
Today, Adaptive received FDA clearance for the clonoSEQ® Assay to assess MRD in CLL, expanding the existing label to a third indication – and providing an important advancement for this community. It is the first and only FDA-cleared in vitro diagnostic for MRD monitoring in CLL, with the ability to measure 1 cancer cell among 1,000,000 healthy cells. This next-generation sequencing assay identifies the genetic sequence for each patient’s unique T or B cell cancer, and then counts the number of these cancer cells when needed, during and after treatment.
This clearance comes at a pivotal time. As newer CLL therapies drive deeper response, MRD testing is increasingly important to assess depth and durability of response. The FDA’s decision was based on samples and outcomes data from two clinical trials which demonstrated:
• CLL patients with undetectable MRD (U-MRD) as measured by clonoSEQ had significantly reduced risk of disease progression compared to patients who did not reach U-MRD status. Patients with U-MRD (MRD < 10-5) by clonoSEQ had a nearly 7-fold decreased risk of disease progression, compared to MRD-positive patients (MRD ≥ 10-5).2 • clonoSEQ MRD results were significantly predictive of progression-free survival (PFS) in both blood and bone marrow samples, regardless of the threshold at which MRD was assessed.2
The CLL treatment landscape has changed dramatically in the last decade, with many new therapies available and a host of promising treatments on the horizon. Patients are living longer because of these advancements and as a result, clinicians need new ways to more accurately assess efficacy earlier in the patient’s treatment journey, either on approved therapies or in clinical trials for new drugs in development.
While clonoSEQ has been used for quite some time from a patient’s bone marrow in multiple myeloma and B-cell acute lymphoblastic leukemia, today’s additional indication in blood as well as bone marrow for CLL patients provides that patient population options for assessing MRD. Blood-based testing, available for the first time as an FDA-cleared use of clonoSEQ, provides patients and healthcare providers with a more convenient and less intrusive option to detect and monitor disease. This is especially advantageous during the time of COVID-19; as we all know too well, cancer doesn’t stop for anything, even a pandemic.
We believe that the value of knowing your clonoSEQ MRD status can be valuable to any patient with these types of blood cancers. To ensure patients have access to testing, Medicare coverage for clonoSEQ was expanded to include testing for patients with CLL in addition to patients with myeloma and ALL. The Medicare CLL coverage policy closely aligns with CLL clinical practice guidelines and supports testing in both blood and bone marrow at time points throughout a patient’s treatment.
There is no easy way to get through a cancer diagnosis and journey. But the ability to know how many cancer cells remain during and following treatment can bring peace-of-mind during a very stressful experience. We are humbled to play a small role in helping to improve patient care in this meaningful way.
May 7, 2020
Announcing ImmuneRACE – A Call to Patients and Survivors to Help Us Crack the Code to COVID-19
Lance Baldo, Chief Medical Officer
Countless people and organizations around the world – from those on the front lines, to those in the lab, to those in the home office – are in a race. Not in a race against each other, but in a race to find solutions to better detect, treat, and contain COVID-19 and ultimately, allow society to reopen safely.
This week, Adaptive Biotechnologies and Microsoft launched ImmuneRACE, a virtual clinical study to decode patients’ immune response to COVID-19. If you are currently fighting, have recently recovered or have been exposed to the virus, your immune system holds important clues about how to detect and fight this disease. By capturing these important lessons learned, we can potentially develop new diagnostics and therapeutics that leverage our bodies’ natural immune response.
Right now, the world needs more reliable testing for COVID-19. Currently there are two types of tests. The first is a PCR test that looks at the virus itself through a nasal swab, and the second is a serology-based blood test that looks at the presence of antibodies in your immune system. But there is potentially a third type of test that looks at a different component of the immune system.
Specifically, the test that we are developing will measure the presence of T cells in the immune system, which identify the disease early on and multiply to combat the infection. By creating a diagnostic that looks at the T cells, we hope to be able to:
Detect the virus in patients that have mild symptoms or are asymptomatic
Determine who may have more severe symptoms and require hospitalization vs. being able to recover at home
Determine if people have or have had the disease, even if antibodies are not present
We are hopeful that this data will be used to help contain the spread of COVID-19, ensure the care matches people’s needs, and ultimately help to reopen society.
Fortunately, the approach we are taking is not new to Adaptive or Microsoft. We partnered more than two years ago to map the immune response of T cells to many diseases, including infectious diseases like Lyme disease, autoimmune diseases and cancers. This effort is an extension of that existing partnership where we are now applying our combined expertise to address COVID-19 and fulfill the need for more reliable testing.
While many people are feeling powerless during this uncertain time, those who have been affected by COVID-19 have an opportunity to make a real difference in the lives of others. If you have or had COVID-19, your immune system has a critical story to tell us about how to beat the virus. We want to learn from you, so together, we can overcome this pandemic.
COVID-19 will likely become part of our lives for the foreseeable future. For that reason, we need many different solutions – preventative, diagnostic and therapeutic – to contain and manage this disease at a global scale for years to come. That’s why we are also making data from ImmuneRACE freely available to public health officials, academia, and the biopharma industry to help accelerate other solutions.
We’re looking forward to seeing and applying the results of our ImmuneRACE Study to inform faster vaccine development, better therapeutic development and more reliable testing. Thank you to everyone who has joined and will join our race and others. It’s going to be the collective efforts of all of us that will lead us toward the finish line.